




ILRI and FANRPAN test nutrition data collection in rural communities using pictography
This blog was written by Vincent Alulu and edited by Paul Karaimu and Judy Kimani.
Have you heard that one must be literate to use the many data collection tools and applications that exist today? That the end user must be at least semi-literate to use such applications to monitor nutrition, and health and fitness, for example? As Vincent Alulu, a research officer with the Sustainable Livestock Systems (SLS) program at ILRI, explains, some data collection tools and technologies have evolved to the point where they can now be used even by those who are not formally educated.
In mid-July 2019, Bertha Mkandawire, a nutrition technical advisor working with the Food Agriculture and Natural Resources Policy Analysis Network (FANRPAN) and I set out from Nairobi to Maralal, an urban centre in Samburu County, which is about 350 km north of Nairobi. FANRPAN and ILRI are collaborating in the ‘Improving Dietary and Health Data for Decision-making in Agriculture and Nutrition Actions in Africa’ project, which is developing, evaluating and introducing cost-efficient and scalable solutions for measuring dietary intake and health indicators to track nutrition and health outcomes and their progress at community and national levels in Kenya.
The initiative seeks to bridge an existing information gap; the lack of affordable, accurate, and reliable information on nutrition and health in Africa, which is home to more than a third of the world’s stunted children. To do so, the project is developing a reliable, low-cost and flexible approach for caregivers and community health volunteers (CHVs) to collect and submit high-resolution dietary, nutrition and health data on children. As such, we were on our way to pilot the proposed solution, a mobile application known as ‘Mbiotisho’, which means ‘Our health’, in Kenya’s Samburu County, one of the country’s arid and semi-arid counties.
Most of the residents in the county are pastoralists who seldom have access to such innovations and have low literacy levels. Rolling out health and nutrition applications in such areas is often difficult largely due to the steep learning curve and sustainability concerns involved in using such applications. To address these challenges, we ensured that the cost of collecting and submitting data with the health application was low by using a short and precise survey and eliminating the need of enumerators. The survey tool we developed uses symbols (pictography) and audio rather than written words so that data can be easily and successfully completed by caregivers regardless of their literacy levels. During the 12-month pilot phase, caregivers will collect high-frequency information on themselves and their children, while CHVs will collect the same information on the same individuals at the standard one-month frequency. Comparisons will then be made between the caregiver-collected data and the CHV-collected data to determine the accuracy of the caregiver-collected data.
‘Mbiotisho’ is a set of two mobile-based applications (on the Android mobile operating system)—one for CHVs and one for caregivers—created on the Logiak platform through a collaboration between ILRI and FANRPAN. The CHVs’ application provides text-based tools for caregivers and child registration, checkups, and performance tracking. Checkups are intended to be collected monthly when CHVs perform their standard households checks, tracking clinical symptoms, consumption and measuring children mid-upper arm circumference (MUAC). The caregivers’ application collects the same information as the CHVs checkup tool but uses symbols and audio-based questions. The caregivers’ interface also has a dissemination tab that, once finalized, provides the caregiver with advisories in response to reported MUAC and dietary diversity score.
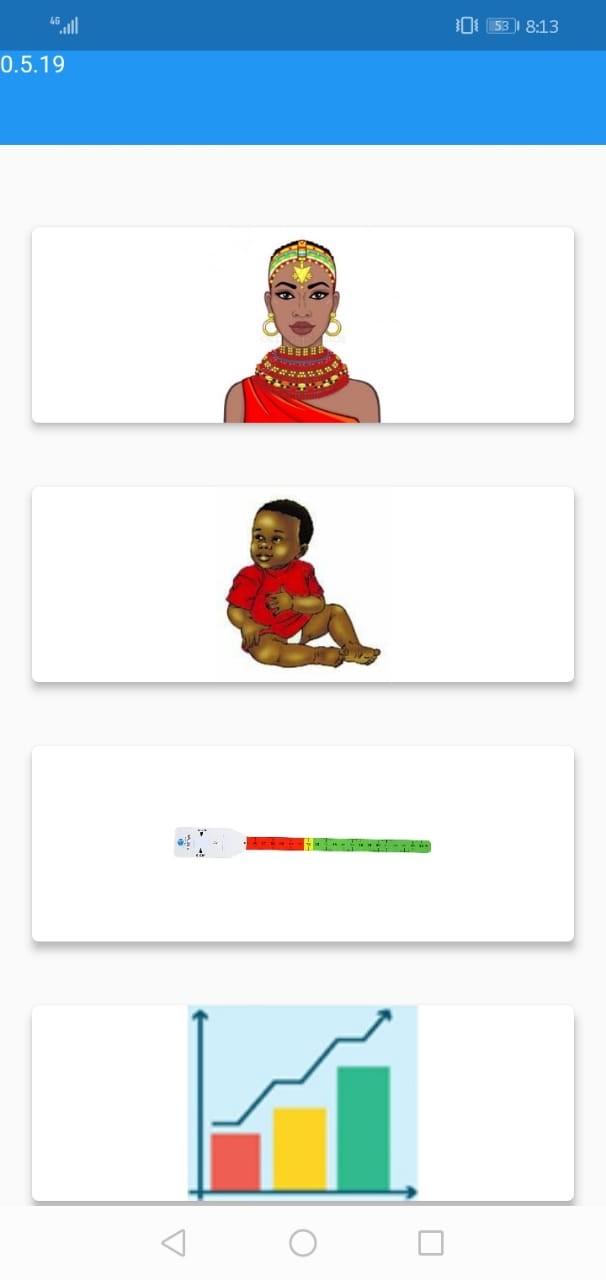

Screenshot: Mbiotisho landing page Screenshot: Mbiotisho child check-up consumption question (photo credit: ILRI).
We envision the data being used not only for assessing the impacts of programming and making timely and strategic area-specific interventions, but also for the longer-term health policies by the local health departments and central government. Data-driven evidence is critical to effective health policy.
A group of 12 participants, 8 of whom were caregivers, accompanied by at least 1 child, and 4 CHVs welcomed us to Lolmolog for the training on 18 July. Watson Lepariyo, a research associate with the SLS program at ILRI, facilitated the first meeting between the project and the participants. We expected the caregivers to have low literacy levels and indeed, we soon learned, most of them could not read or write. Armed with this understanding, we hoped to effectively introduce the application and train them on using it with the help of CHVs.
 Training in session at Lolmolog (photo credit: Vincent Alulu/ILRI).
Training in session at Lolmolog (photo credit: Vincent Alulu/ILRI).The training and practice sessions focused on ensuring participants mastered the routine questions on consumption and measuring MUAC to enable them collect the same data at stipulated times. Our aim was to learn the extent to which caregivers could successfully collect and submit data using the application, and receive feedback on how to improve it.
On the first day, we invited the participants and their spouses to explain and emphasize their role in the exercise, as well as to share the background and goals of the research project. We then distributed smartphones and instructed them on their basic functionalities and trained the CHVs on the data collection application. The project also provided participants with solar chargers for charging the smartphones given that the area is not connected to the national electricity grid but has plenty of ‘green’ energy that can be harnessed using the solar chargers.
The second day began by registering caregivers on the application and training them on how to use the phones. Lepariyo led the session in the local dialect using his own gadget while participants followed on theirs. The enthusiasm was palpable as he demonstrated how to use application on the phones and how to take photographs. After the demonstration, the caregivers could locate the camera application and take photographs of their fellow participants and children! Considering the participants’ low literacy levels and near complete lack of experience using smartphones, we were pleasantly surprised that they so easily grasped how to use the application.
We then moved on to showing them how to use the data collection component of the application. We also taught them how to turn on cellular data and GPS location features which would be key in data submission and geotagging the data submitted, respectively. Since these two were easily grasped, we let them practice locating the application and turning data and location features on and off.
The caregivers were eager to learn and test their knowledge through a few assignments on navigation and basic phone use. We were all pleased. What seemed to us a daunting task at the start, was looking doable. To test their understanding so far, Lepariyo opened his caregiver nutrition application and this time asked the participants to do similarly. They all did. We had none to assist!
Lepariyo then went through the application, explaining the questions and responses that each icon represented. The application has questions related to dietary diversity, which rely on icons to represent food groups. He ensured the women understood the food groups and could correctly classify common foods. He also trained them on measuring their children’s MUAC, an indicator of nutritional status, and how to take a picture using the application. This was the critical part of the training because accurately measuring MUAC requires a fair degree of precision and taking a picture of the child’s arm with the MUAC band on it is challenging. I logged into the back-end of the application to check the data that had been submitted and saw that each of the phones had uploaded data. Gratified with the accomplishments of the day, participants went home with the phones to practice further.
We ended the day relieved but not fully satisfied because we suspected that some participants might have been soliciting help from fellow participants during the practice sessions. The jury was still out on whether each of them could successfully use the application. We needed to wait until after the weekend too see how much they could remember and do on their own.
 Photo of the participants and their children (photo credit: Vincent Alulu/ ILRI).
Photo of the participants and their children (photo credit: Vincent Alulu/ ILRI).On Monday the following week, after the caregivers had spent the weekend using the phones on their own, we assessed what they had learned during the training and practice at home. We listened to their experiences and shared troubleshooting tricks. We were all happy with the progress, having looked at the data submitted over the weekend, though we believed the caregivers could do better, especially in improving the quality of pictures. We repeated the training on tying the MUAC band and taking pictures to extract accurate MUAC measurements, which improved the quality of subsequent pictures.
This first visit and training session was an invaluable experience that gave us practical knowledge on some of the challenges that we will likely face during the main implementation of the project. This information will be used to ensure the roll out of the application in the last quarter of 2019 goes smoothly. Importantly, our fear that the caregivers’ low literacy levels and lack of smartphone experience would limit their ability to use the application was dispelled.
Our next step is to use the lessons learned from this pilot to improve the usability of the application and then begin preparing for the main implementation, which will include 180 caregivers and 20 CHVs.
We would like to thank the International Development Research Centre for funding this activity and the forthcoming implementation phases.
More on this and related project activities and information can be accessed at https://www.drylandinnovations.com/healthandnutritiondata

")

..")










